Infants Part I (1 Hour)
Now that you are prepared to actually get in the door and perform an assessment, the next difference you will have to overcome are anatomical. Let’s start with the head.
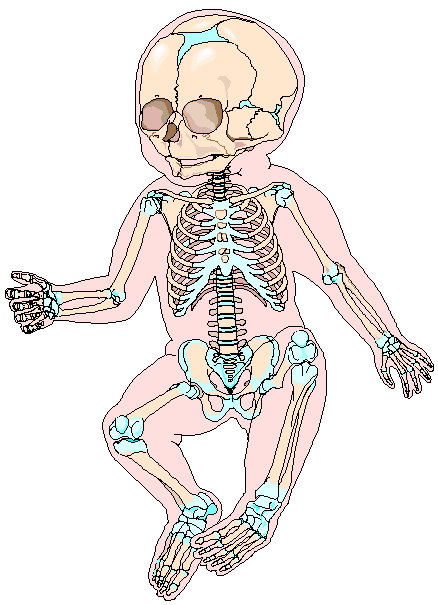
The first thing you should notice about the head is that it is huge for the size of the baby. The neck has to develop in order to control the head, which is why the head must always be supported when you pick up an infant. To facilitate the delivery of the baby, the baby’s head was designed with natural relief points built in called the fontanelles. The fontanelles are literally holes in the infant’s skull. The skin on the infants head is nearly the only thing separating you from the infant’s brain (save for meninges, dura mater, etc.). Given the size of the head and the weakness of the neck, maintaining a neutral position of the neck becomes a high priority. The head is large and cumbersome, to the point where the weight of the head can fall forward creating a kink in their already weak necks. For this reason you are taught to place padding underneath the shoulders when immobilizing the patient or maintaining an airway. The vulnerabilities listed above (weak neck + big head) place the infant at greater risk for c spine and head injuries. Positioning the head and maintaining the neck in a neutral position are keys in maintaining the infant airway.
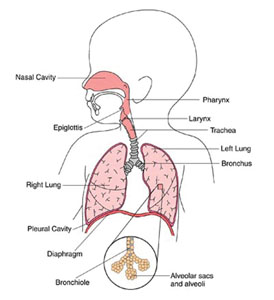
As we examine the infant airway, the first thing you will notice is the size. Everything is smaller. The structures of airway (epiglottis, larynx, and trachea) are smaller versions of the adult airway, which make them prone to foreign body airway obstructions (not to mention the tendency of the infant to put things in their mouths). Conversely, the tongue is much larger in terms of surface area when compared to the adult airway and can easily become an obstruction (worse than in adults). Infant teeth tend to be easily dislodged in the event of facial trauma and pose an obstruction hazard. The neck is shorter; however the trachea is very narrow. The narrow trachea is a problem for even the healthy infant since birth when you consider how difficult it is for them to control their head. To make matters worse, the trachea is very flexible. These properties, when combined with the narrowness of the trachea, make it easy for the infant to ‘crimp’ the trachea by virtue of their head position. This tendency for the trachea to ‘crimp’ affects how you hold the infant. When picking up an infant, ensure that you support the head and place it in a neutral position. Infants also produce greater amounts of secretions. Given all the variables mentioned above, have a more difficult maintaining their airway. Infants are also obligate nose breathers. This means that if suctioning is to be performed, remember to suction the nose as well. Being able to manage these small and disproportionate airways will pay great dividends when assessing and managing the infant airway.